Cyanotic congenital heart disease is a collective name for a group of heart defects at birth or neonatal stages which results in deoxygenated blood entering systemic circulation (the process of carrying blood to and fro through your body). The oxygenated and deoxygenated mixture circulated in the body leads to cyanosis – blue coloring of the skin, visible particularly on the lips, toes and fingers. Though most of the cases of cyanotic CHDs have genetic roots, there are some with external influences.
Types of Cyanotic Congenital Heart Disease
Cyanotic Congenital Heart Disease is caused by various physical defects of the heart like malposition of the great arteries, bidirectional shunting and others. These various defects are used to further classify the Cyanotic CHD according to the physical defect causing it.
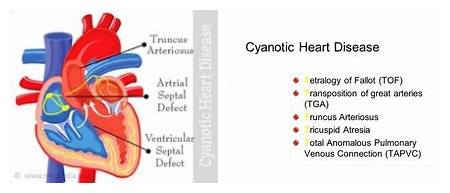
Tetralogy of Fallot (ToF)
The name itself suggests that ToF is a combination of four different defects – narrowing of the right ventricular outflow tract between the two bottom chambers of the heart, thickening of the right ventricle causing boot-shaped appearance and aortic valve with biventricular connection. It was described by French physician Etienne-Louis Arthur Fallot in 1888.
Total Anomalous Pulmonary Venus Connection (TAPVC)
TAPVC is a complication which occurs when pulmonary veins which carry oxygenated blood from the lungs to the heart are malpositioned to the right atrium. Ideally, the pulmonary veins are connected to the left atrium which then pumps this oxygenated blood to the rest of the body. There are four variants of this disease – Supracardiac, Cardiac, Infradiaphragmatic and a mixed variant.
Transposition of the Great Arteries (d-TGA)
TGA is a part of the congenital heart defects family where the primary arteries switch positions. The switching of positions leads to pumping of the deoxygenated blood in to the body instead of lungs.
Pulmonary Atresia (PA)
The congenital malformation of the pulmonary valve where the orifice fails to develop is known as Pulmonary Atresia (PA). The pulmonary valve has three flaps which act as a one way door that pushes blood flow to the lungs, but prevents any backflow from the lungs into the right ventricle. The thickening of this valve blocks the opening and prevents blood flow from the pulmonary artery to the lungs. This condition does not affect a developing fetus as oxygen is acquired from the mother’s placenta. However, blocking of the pulmonary artery because of PA in newborn babies causes them to turn blue in color.
Tricuspid Atresia
This congenital defect is caused by the abnormal formation or complete absence of the tricuspid valve in the right atrium which results in an undersized or absent right ventricle. Because of this defect, the heart is not able to properly oxygenate the body. The lack of oxygen caused by this defect can turn fatal for newborns suffering from this condition.
Common Symptoms
The most commonly visible symptom of Congenital Heart Defects is cyanosis – the blue coloring of the skin, specifically on the lips, toes and fingers. Dyspnea – a breathing problem encountered by children after physical activity. Other common symptoms observed during spells of oxygen deprivation include sudden increase in the bluish color of the skin, hyperventilation and anxiety attacks. Crying and irritability are the two major behavioral indications of CHDs. Specific symptoms are observed depending on the type of physical defect affecting the patient.
Tetralogy of Fallot (ToF)
- Low birth weight
- Rapid Breathing
- Difficulty in feeding
- Heart murmur (the sound intensity varies from imperceptible to incredibly loud)
- Clubbing of fingers and toes
- Retarded growth and physical development
Total Anomalous Pulmonary Venus Connection (TAPVC)
- Rapid breathing
- Rapid heartbeat
- Slow growth
- Chronic respiratory infections
- Cynosis
Transposition of the Great Arteries (d-TGA)
- Heavy sweating
- Rapid breathing
- Rapid heatbeat
Tricuspid Atresia
- Cyanosis
- Chronic respiratory infections
- Heavy sweating
- Tiredness
- Shortness of breath
- Difficulty in feeding
Diagnosis
Diagnosis of cyanotic CHDs is classified into two main subtypes depending on the occurrence of the defect.
Prenatal Diagnosis
Depending on the gestational age, fetal position, type of defect and expertise of the operator, prenatal sonograms can identify structural malformations of the heart. Detecting heart defects using fetal echocardiography is not always possible.
Postnatal Diagnosis
Various tests both invasive and noninvasive are part of the postnatal diagnosis to detect CHDs.
1. Physical exam
A physical exam might be conducted to check for cyanosis and clubbing both of which are major symptoms of CHDs.
2. Echocardiography
In this test, high frequency sound waves are used to create an image of the heart. This test is conducted post birth as some defects missed during the prenatal test might be detected later as the heart develops.
3. Chest X-ray
A chest X-ray is used to reveal presence of any excess amount of blood in the lungs or the unusual appearance of the heart as both are signs of heart disease.
4. Electrocardiogram
Electrical activity of the heart is measured in this test with the help of electrodes placed on the skin around the heart. The electrical activity of the heart is measured to evaluate its beating with the help of a computer.
Treatment
Treatment for Cyanotic Congenital Heart Disease depends on the type of the disease affecting a patient. The treatment procedure can be short and simple or long-term and complicated, involving surgery.
Tetralogy of Fallot
The narrowing in pulmonary valve and the hole in the heart can be treated only with surgery. Heart surgery on infants is a bit risky and hence, if the symptoms are not very severe, your doctor might postpone the surgery for a later date of three to six months. If the symptoms are severe, immediate surgery might be recommended.
Total Anomalous Pulmonary Venus Connection (TAPVC)
TAPVC can be corrected with surgery by adjusting the malpositioned veins to their appropriate position in the left atrium. Surgery can be scheduled at a later date if there is no blockage in the pulmonary vein.
Transposition of the Great Arteries (d-TGA)
A catheter might be used to create a temporary hole in the atrial septum (the upper dividing wall of the heart) which encourages mixing oxygenated and deoxygenated blood. Single ventricle defects will be treated with an injection of prostaglandin.
Tricuspid Atresia
The first step of treatment involves an injection of prostaglandin which facilitates the mixing of oxygenated and deoxygenated blood. The next step is to create an artificial passage between the heart and the lungs called as the shunt. The next stage involves connection of the deoxygenated blood carrying veins of the upper body to the pulmonary valve. The last stage involves connecting all the remaining veins to the pulmonary valve. Due to the complexity of the treatment process it progresses at fixed time intervals.
